Scientists from the International Centre for Translational Eye Research (ICTER) have undertaken the challenge of creating diagnostic technology that could prove to be fundamental for the understanding of eye diseases. Their solution will aid in the rapid diagnosis of conditions such as age-related macular degeneration (AMD), inherited blindness, diabetic retinopathy, or retinal vascular occlusion.
The team of scientists at ICTER introduced a new functional imaging method called flicker-based Optoretinography (ORG). With this technique, nanometer-long changes in the length of photoreceptors associated with the vision process are recorded. The baseline technology behind our ORG is Spatio-Temporal Optical Coherence Tomography (STOC-T). ORG will enable ophthalmologists to diagnose diseases much faster and more effectively than today. Most importantly, the examination involving the patient will take just one-hundredth of a second.
Whole-eye optical coherence tomography (OCT) imaging is a promising tool in ocular biometry for cataract surgery planning, glaucoma diagnostics and myopia progression studies. However, conventional OCT systems are set up to perform either anterior or posterior eye segment scans and cannot easily switch between the two scan configurations without adding or exchanging optical components to account for the refraction of the eye’s optics. In this work, we present the design, optimization and experimental validation of a reconfigurable and low-cost optical beam scanner based on three electro-tunable lenses, capable of non-mechanically controlling the beam position, angle and focus. The proposed beam scanner reduces the complexity and cost of other whole-eye scanners and is well suited for 2-D ocular biometry. Additionally, with the added versatility of seamless scan reconfiguration, its use can be easily expanded to other ophthalmic applications and beyond.
Text: Dr. Andrea Curatolo – Principal Investigator in the IDoc group at ICTER.
Publication:
María Pilar Urizar, Enrique Gambra, Alberto de Castro, Álvaro de la Peña, Onur Cetinkaya, Susana Marcos, and Andrea Curatolo, “Optical beam scanner with reconfigurable non-mechanical control of beam position, angle, and focus for low-cost whole-eye OCT imaging,” Biomed. Opt. Express 14, 4468-4484 (2023)
Ophthalmology is one of the fastest-developing fields of medicine. This is only possible by improving existing procedures and developing new eye treatment methods. We discuss the importance of the continuous development of ophthalmic techniques with Dr. Piotr Chaniecki.
What is the most crucial aspect of ophthalmology for you?
PC: Ophthalmology relies on technology. The most significant advancements in this field occurred after developing diagnostic devices and surgical techniques. The level and improvement of technology directly influence the precision of procedures and the effectiveness of direct diagnosis. The International Center for Translational Eye Research (ICTER) is focused on developing such devices. I see tremendous potential in creating new tools for doctors that will contribute to better and faster diagnoses.
As seen in Western clinics, ophthalmology in Poland is developing rapidly, but we still have a long way to go regarding technological advancement.
Why is the lack of specialized research being conducted in Poland that could help patients?
There is still much to be done. We are not lacking specialists, and I take pride in having trained several ophthalmologists, surgeons, and diagnosticians who now work as independent and excellent doctors in Polish clinics. In Poland, I observe a kind of stratification, with some places offering diagnostics and treatment at the highest global level while others require significant investment. Money is, of course, a problem, but not the only one – there is a lot of equipment in Polish facilities that is not always fully utilized. What is the reason for this? I can only speculate that it is due to a lack of ideas about how the equipment can be used for research, or perhaps it is due to a persistence in established procedures and routines. What I sometimes notice in conversations with doctors, including those working in academia, is a reluctance to change and challenge the status quo – if a diagnostic method works, why change it? If we can make a diagnosis based on average-quality results, why bother striving for more? Additionally, the entire system of training doctors requires many changes.
I can’t entirely agree with such an approach, which is one of the reasons I decided to collaborate with ICTER, as it holds great potential for the benefit of patients.
Dr. Piotr Chaniecki
From a clinical perspective, what equipment developed at ICTER is the most important?
My research shows many devices with enormous potential to improve surgical procedures. I firmly believe that some of them will be “milestones in global ophthalmology.” This is not art for art’s sake. Better equipment and technology mean better diagnostics and increased patient safety during surgical procedures. I’m referring to the possibility of reducing the number of complications in surgical techniques and increasing the accuracy of diagnoses. As an experienced ophthalmologist who performs procedures according to the highest standards, I know the criteria will be even more demanding.
What are the numerical occurrences of complications in your practice?
Complications are a particularly challenging topic for every doctor. Every active surgeon encounters complications, so it is true what they say, “those who don’t operate don’t have complications.” Complications can be considered statistically, but one must approach the numbers cautiously. Even Mark Twain wrote about statistics, stating there are three kinds of lies: lies, damn lies, and statistics.
When looking at complications numerically, one would need to consider a specific procedure, such as cataract surgery. Here, sources provide values ranging from 0.3% to 15% of cases, depending on the complexity of each case. I consider complications as lessons from which I continually learn. My statistics regarding complications are within the lower range of the statistical scale.
Congratulations.
This largely depends on accuracy, which is also influenced by technology. Technology developed at ICTER will undoubtedly contribute to reducing the number of complications during surgical procedures. Another area where I see tremendous potential is diagnostics. Advanced technology will certainly increase the accuracy of diagnoses and allow us to view a given pathology from a broader perspective. Wanting to cure a patient is not enough; we must first know what to treat.
How many cataract removal surgeries with intraocular lens implantation are performed in Poland?
In Poland, approximately 300,000 such surgeries are performed annually. Worldwide, around 20 million lens implantation procedures are carried out. These numbers have fluctuated significantly over the past three years due to COVID and geopolitical circumstances.
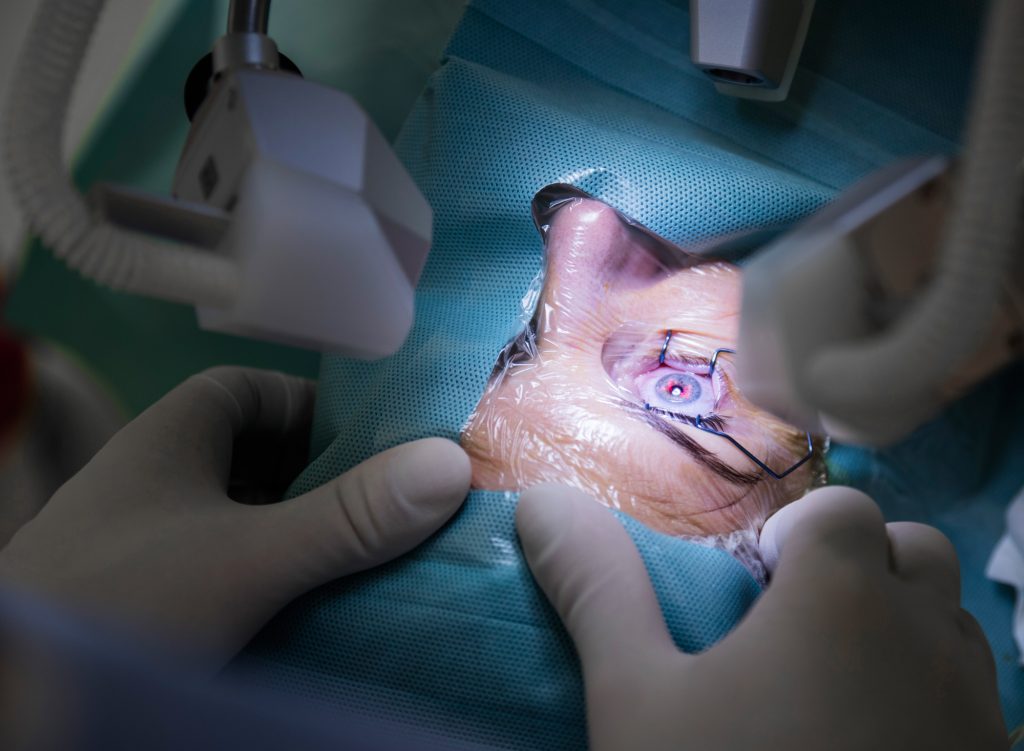
Ophthalmic surgery at an eye clinic
Gene therapy is another area being developed by ICTER. What prospects do you see there?
Gene therapy primarily offers a chance for visually impaired patients due to genetic disorders, such as those suffering from Leber congenital amaurosis (LCA). In individuals affected by LCA, the eye’s photoreceptors stop responding to light due to a mutation in the gene that codes for a protein essential in the visual process. Total blindness occurs around the age of 20. Research on gene therapy to remove or alleviate LCA symptoms has been ongoing for almost 15 years, and a viable treatment may soon be available. It is research institutes like ICTER that enable such progress.
Does gene therapy have a chance to become established in Polish medicine in the next few years?
We need to approach this topic realistically. Bringing a drug to market costs hundreds of millions of dollars. Research at each stage, including clinical trials, animal models, healthy volunteers, and patients, takes significant time. We are talking about a period of 5-10 years.
In addition to the research you are currently involved in with our scientists, focusing on patients with multiple sclerosis, do you plan to expand our collaboration to include patients with other conditions?
Indeed, in the next stage, we could involve age-related macular degeneration (AMD) patients. I see potential in diagnosing, monitoring disease progression, and assessing treatment effectiveness. Existing devices allow for structural imaging, which shows anatomical changes in different layers of the eye. Still, they do not provide functional imaging, meaning we cannot determine the state of crucial substances involved in vision biochemistry. Therefore, sometimes successful surgery does not result in improved vision for the patient. Such situations could be avoided if we knew beforehand whether the part we intend to repair is functioning. And this is where I see enormous potential in collaborating with the International Center for Translational Eye Research.
We want to benefit from your experience in ophthalmic practice, as it can help us refine the equipment we are developing. Do you have any guidance for us at this time?
First and foremost, for any device to be introduced into medical offices and operating rooms, it must be practical and user-friendly. It is not about the simplicity of the design or the principle of operation— not everyone needs to know how something works. Many people need to be able to operate the device. ICTER has developed many devices, such as systems for assessing retinal receptor function, which, with the suitable “packaging,” could quickly be implemented in clinics. The key is to create appropriate software so that the equipment can be operated by technicians or doctors after brief training without the need for an engineer. The second aspect is ergonomics and comfort for the patients. Let’s not forget that most patients are elderly individuals who may have mobility issues, not to mention spending 20 minutes in an immobile position during an examination. Additionally, some procedures can be particularly frustrating for them, primarily when they must focus on a bright spot they cannot see due to diseased changes in the retina. My goal is to present the clinical perspective to scientists.
Aside from my absolute satisfaction, our collaboration will benefit the patients the most. The fusion of technology, medicine, science, and practice always benefits all parties. The same will be confirmed in our case. I am eagerly looking forward to the results of this collaboration.
As are we.
Thank you for the conversation.
BIO
Piotr Chaniecki currently serves as the Chief Surgeon at the Prof. Zagórski Eye Surgery Center in Krakow. His professional background includes graduating from the Military Medical Academy in Łódź in 1996. He has also held the position of Head of the Clinical Ophthalmology Department at the 5th Military Clinical Hospital in Krakow and the Ophthalmology Department at the PCK Hospital in Gdynia. His main areas of professional interest are anterior and posterior segment eye surgery, as well as conservative treatment of eye diseases. He is the author of a unique technique for intraocular lens exchange, which was recognized as the best surgical technique of 2019 by the American ophthalmic journal Cataract & Refractive Surgery Today. In 2016, he received the award for the best scientific paper titled “Composition of phacoemulsificated human lenses analyzed by infrared spectroscopy,” presented by the European Association for Vision and Eye Research.
An interdisciplinary team of world-class scientists at the International Centre for Translational Eye Research (ICTER), operating at the Institute of Physical Chemistry of the Polish Academy of Sciences (IPC PAS) in Warsaw, is working on technologies that will revolutionize the diagnosis and treatment of the most challenging eye diseases. On May 10, 2023, journalists were able to learn about the centre’s achievements and talk with researchers. Ambassador of the United Kingdom of Great Britain and Northern Ireland to Poland Anna Clunes was the event’s guest of honor.
The International Centre for Translational Eye Research (ICTER) was established thanks to European funds from the Intelligent Development Program (POIR) awarded by the Foundation for Polish Science (FNP) under the International Research Agendas (MAB) program. The research carried out in MABs is interdisciplinary in nature and the results will enable the development of new technologies to serve society in the future.
– “ICTER is one of 14 International Research Agendas. It is the only such program in Poland, which allows the creation of new research units led by outstanding scientists” – explained FNP Vice President Dr. Tomasz Perkowski, adding: – “The aim of the International Research Agendas program is to strengthen the quality of science in Poland, develop international cooperation and attract talent, and support the creation of innovative, internationally competitive solutions in a given field.”
Dr. Tomasz Perkowski – Vice-President of the Foundation for Polish Science.
Researchers at the centre are working on breakthrough technologies for imaging eye processes and facilitating procedures to save or restore vision. Research is interdisciplinary in nature and involves areas such as biology, chemistry, physics and computer science. At ICTER, one-third of the scientific staff are foreigners. – “For centuries, treating blindness was considered a miracle. Now there are emerging opportunities to treat even people who have been blind since birth. This shows how far we can go in treating eye diseases” – said Prof. Maciej Wojtkowski, director of the ICTER – IPC PAS.
Some of the technologies developed at the ICTER are at the implementation stage. One of them is an innovative method that allows imaging of the retina using so-called fluorescence with two-photon excitation. It allows, on the smallest, chemical scale, to check whether the cells responsible for the vision process are working properly. Another method is optoretinography, which allows precise measurement of the response of photoreceptors present in the retina to light. Both techniques can be used to diagnose visual disorders, but they also make it possible to analyze whether implemented therapies are having the intended effect. In the case of optoretinography, the technique requires previously unimaginable precision – measuring devices must detect the elongation of light-sensitive eye cells by 1 nanometer, despite the movement of the entire organ.
Prof. Maciej Wojtkowski – Chair of ICTER.
ICTER collaborates with the world’s leading eye research institutes, including University College London – the centre’s strategic partner – as well as London’s Moorfields Eye Hospital and the University of California, Irvine. – “International scientific collaboration is key to advancing science and innovation, as well as to solving global health, climate or security challenges. Scientific cooperation across borders allows for the expansion of knowledge by additional elements, exchange of experience and competencies, access to research infrastructure and technology transfer” – said Anna Clunes, Ambassador of the United Kingdom of Great Britain and Northern Ireland to Poland, adding: – “The UK is an active partner of Poland in the field of scientific research. I am pleased that British centres and ICTER maintain close cooperation in research on the eye and its diseases. This is an important area for improving the quality of life for millions of people around the world. I hope that this cooperation will grow and benefit all countries.”
Anna Clunes, Ambassador of the United Kingdom of Great Britain and Northern Ireland to Poland and Prof. Maciej Wojtkowski.
The support of the Foundation for Polish Science in the implementation of the International Research Agendas program is not only an opportunity for the development of domestic science – in perspective, it means an increase in innovation in the Polish economy. Technologies being developed and tested in MABs today, in a few years’ time, may have a significant impact on various branches of our economy, and this will translate into concrete benefits for society. In the case of ICTER, the new devices will be used to test innovative therapies for, among others, patients with diabetic retinopathy, which is the first cause of vision loss in people of working age, or with age-related macular degeneration (AMD), the most common cause of vision loss in people over 50 in developed countries.
Director Kinga Słomińska, Foundation for Polish Science.
***
The Foundation for Polish Science has existed since 1991 and is an independent, self-funded, non-profit, non-governmental institution with a mission to support science. It is the largest non-budgetary source of science funding in Poland. FNP’s statutory goals include supporting outstanding scientists and research teams and working to transfer scientific achievements to economic practice. The Foundation pursues them by awarding individual prizes and scholarships for scientists, granting subsidies for the implementation of scientific achievements into economic practice, other forms of support for important undertakings serving science (such as: publishing programs, conferences). The Foundation is also committed to supporting international scientific cooperation and enhancing the scientific independence of the younger generation of scientists.
***
Pictures from the event: Nel Gwiazdowska
PR coverage of the media conference: Pełka and Partners agency
***
Press contact:
Dominika Wojtysiak-Łańska, Foundation for Polish Science: tel. 698 931 944, wojtysiak@fnp.org.pl
On May 09, 2023 we hosted Optica’s Director for Europe, Dr. Claus Roll, at ICTER. It was a great opportunity to share with him the achievements of ICTER and talk in detail about the projects we are conducting. First, during the initial presentation, Dr. Andrea Curatolo presented the general goals and scope of the ICTER center, and talked in general about the research work carried out in the IDoc and POB groups. A detailed discussion of the ongoing projects took place during a tour of the laboratories. Piotr Węgrzyn, Wiktor Kulesza and Maciej Wielgo talked about their research on STOC-T. Klaudia Nowacka presented the results of her work on Dynamic Light Scattering (DLS) and the Pi-NIRS method. Jadwiga Milkiewicz and Karol Karnowski talked about the device they constructed (as part of the Imcustomeye project) to study corneal biomechanics. Then again Karol Karnowski together with Krzysztof Gromada presented the image-assisted eye microsurgery platform constructed in IDoc Group. Finally, Marcin Marzejon presented two-photon excited fluorescence systems for mice and humans constructed at POB.
During his visit, Dr. Claus Roll introduced us to OPTICA’s most important areas of activity. One of them is the activities of the Optica Foundation, one of the main goals of which, as Dr. Roll mentioned, is to inspire, support and mentor students and early career professionals who will be the future change-makers in optics and photonics.
Optica’s director explained the offer of scholarships, internships, grants and other activities aimed at the career development of young people. Of particular interest to the ICTER community worth noting are the scholarship that OPTICA provides, including the Chang Pivoting Fellowship, where individuals can apply for unrestricted funds to pursue a new passion related to optics and photonics, or the Deutsch Fellowship, a fellowship in partnership with the Wellman Center for Photomedicine at Massachusetts General Hospital.
The meeting was also an opportunity to talk about the CRATER conference, which ICTER is organizing in early September 2023.
***
Text: Katarzyna Wybrańska, PhD – IDoc’s group Coordinator.
The Conference on Recent Advances in Translational Eye Research 2023 (CRATER 2023) is a platform for all researchers, investors, and entrepreneurs whose interests focus on the eye, to meet and discuss frontiers of the research, commercialization, and translation of the studies. The first edition of the CRATER, prepared by members of the ICTER community, will be held in Warsaw on 7-8 September 2023 in Copernicus Science Center.
The conference will provide space for discussion between specialists from different fields who are united in their pursuit to understand better the challenges of eye imaging, the process of vision, and formation of eye diseases. During this international and interdisciplinary event, participants will discuss frontiers of research on new methods and tools enabling diagnosis and treatment of eye diseases and also ideas on how to facilitate rapid implementation of new eye therapies.
Detailed information on the conference’s, including a list of invited speakers, is available on the conference webpage – crater.icter.pl.
Registration for the Conference on Recent Advances in Translational Eye Research 2023 which is organised by ICTER is already open, with early registration fee available until 30 June 2023. You can contribute to the program and present your research results – the call for abstracts is open until 13 May 2023 (extended deadline).
Dr. Anna Ambroziak is an ophthalmologist specializing in eye diseases with 27 years of professional experience and an Assistant professor at the Faculty of Physics, University of Warsaw. Dr. Ambroziak is a member of the Polish Society of Ophthalmology (PTO) and the Society of Polish Ophthalmic Surgeons (SCOP). Dr. Ambroziak is also the Polish representative in the European Contact Society of Ophthalmologists (ECLSO), lecturer at the European Studies in Ophthalmic Optics and Optometry, and editor of the position paper of the Polish Expert Group of the Academy of Ocular Surfaces.
Dr. Ambroziak has more than 200 publications to her credit. She promotes the idea of interdisciplinary cooperation. She adheres to the philosophy of a holistic approach to the patient. Under her leadership, the Ophthalmic World Eye Center in Warsaw (Centrum Okulistyczne Świat Oka) has won the Health Ambassador Award for its expertise, experience and improvement in patients’ quality of life.
Based on the clinical studies conducted by Dr. Ambroziak, a therapeutic lens made of lotrafilcon A was registered by the US FDA. She is the winner of the ECLSO “Kersley Lecture” grand prize and the Medical University of Warsaw Scientific Award.
Dr. Anna M. Ambroziak
We present an interview with Dr. Anna Maria Ambroziak conducted by the Physical Optics and Biophotonics group at ICTER.
In recent years, the development of cooperation between ophthalmology and optometry in Poland has been noted. ICTER brings together specialists from the fields of optics, optometry, engineering, physics, biochemistry, mathematics to create specific tools and solutions that can translate into improved patient care. How do you think the collaboration of those involved in vision science has been changing in Poland over the past decades?
So, to begin with, a little bit of my personal memories, which will shed some light on the history of optometry in Poland. That is, a few words about how Optometry became the foundation of Ophthalmology in the country on the Vistula River.
In ’98, as a member of the Board of Directors of the Contact Lens Section of the Polish Ophthalmological Society, I organize a meeting, and a few months later a contactology symposium. That’s a little over a year after the first year of optometry postgraduates graduate from the K. Marcinkowski Medical University. The following years saw more conferences. Among the guests invited to the symposium were world-renowned optometrists, contactology experts – including Brian Holden, Lyndon Jones, Philip Morgan, Keith Edwards, Dwight Akerman, Brian Tompkins, Eric Papas and myself – a young ophthalmologist ready to change the world. Since the beginning of my career, I have been involved in the education and development of optometrists. I have been working at the University of Warsaw since 2011, for more than 10 years served as deputy editor-in-chief of the medical journal Contactology and Ophthalmic Optics. I took an active part in such events as the introduction of the world’s first silicone hydrogel lens to the Polish market. My love for contactology exploded suddenly and turned into a mature, fulfilling relationship. Scientific research on the effects of prolonged contact lens wear on the ocular surface became the subject of my doctoral dissertation defended with distinction at WUM. On the basis of clinical studies conducted by me, a therapeutic lens made of lotrafilcon A was registered by the US FDA. To paraphrase a classic, it was worth looking at such a map of the world which includes utopia. For me, there was no dilemma, problem or division. The more I know, the more questions I ask and the more joyfully I share knowledge. In this natural environment of broadly understood vision care, we should work together to best serve each other and our patients. There is no room for divisions here, we are one compatible, integral creation and naturally work together. For a wise scientist, the other person is an opportunity for development and cooperation, and if also for competition – it is only for the positive and constructive one. Years of work and creation of this ideal world have allowed us to raise new generations of specialists, these new generations work with each other and learn from each other. The Ophthalmic Center Świat Oka is a scientific and research & science clinic with modern training facilities, where optometry and medical students learn and work under the supervision of specialists, where clinical trials of drugs and technologies are carried out, and papers and publications are produced, including many on rules of procedure and ophthalmic-optometric cooperation. I strongly recommend this model. There is much work ahead of us, but let’s remember that changing the world should always start with ourselves. I have been supporting the development of Optometry in Poland since the beginning, working as an assistant professor at the Faculty of Physics at the University of Warsaw. In the academic environment of Warsaw, I was the first ophthalmologist to start teaching new generations of optometrists – teaching the younger generations at a proper level should be the primary goal for eye care specialists. I execute the plan according to which the Ophthalmologist and the Certified Optometrist work together on one level. This cooperation is not possible without the presence of scientists from the fields of optics, physics or mathematics, biology and chemistry. Education and Science is the future not only for this country, but for the whole world.
What are the most troublesome diagnostic limitations and needs of a modern ophthalmology center? If you could “conjure up” the equipment of your dreams, what would it diagnose (or what other function would it perform) and how?
Our tears are a vast, still tentatively explored, wealth of knowledge about our organisms enabling us the insight into more than just our genomics, and this is one of the directions I dream of.
Our brains are the realm where perception happens and where reality is created, and we can extend it using artificial intelligence; this is another important signpost for female and male wizard scientists.
The power of now shows, at the same time, a great need to monitor the progression and development of myopia. We know more and more about the effectiveness of the available solutions and are oriented towards polytherapies. We know more and more about new optical designs for eyeglasses and contact lenses, and about the long-standing results of meta-analyses of the use and clinical evaluation of these products. We are definitely vocal about the need to measure the axial length of the eyeball, the need to monitor and treat pre-myopia, and the impact of the pupil width on monitoring the development and progression of myopia. The power of now is also the power of creation, so we keep track of what science brings to practice. For example: Transplantation of embryonic human stem cells into the retinal pigment epithelium (RPE) is happening before our eyes – now in the cases of age-related macular degeneration, but soon in myopic maculopathy. The M1 molecule promotes the regeneration of retinal ganglion cell axons which means the potential to restore the activity of target neurons and thus restore visual function in cases of both maculopathy and neuropathy.
Do you think the demand for devices and techniques for visual system diagnostics will grow in the near future? Why?
The eyesight is the most important sense, but it is subject to a series of involutionary processes and the influence of exo- and endogenous factors. The increase in life expectancy has made the estimation numbers in epidemiology unequivocally indicate the imminent scale of the challenge. Returning to the example of myopia, we know that soon half of the world’s general population will be myopic and thus the number of myopia-related complications will increase, including the most serious and severe myopia-related maculopathy, which does not exclude the coincidence of age-related changes. Prevention based on modern, reproducible, minimally invasive and highly specific diagnostics is the basis of ophthalmology. In addition to the pandemic of myopia, often the same patients due to being overweight and obese add to a growing group of patients burdened with diabetes. In this group, the rise of maculopathy is also a critical challenge.
Online doctor consultations are already exploiting algorithm and data analyses today. Diagnostic tests and therapeutic regimens are becoming more precise, new previously unknown solutions and materials are being used. Technologies using virtual reality are already the foundation of our practice in vision therapy.
Artificial intelligence in the daily work of an eye care specialist involves much more than just monitoring fundus changes or the screening programs we are already familiar with nowadays and that are particularly advanced in the prevention of diabetic changes. The pandemic has brought us new challenges, new goals and new experiences.
Dr. Anna M. Ambroziak with a patient.
Are there eye diseases whose pathogenesis we have yet to understand? Do they occur frequently – affect many people?
As I mentioned, the time of SARS-COV-2 is an acceleration of the development of the implementation of technological innovation and artificial intelligence in medicine. For us, this time is also the intersection of the myopia pandemic, diabetic eye syndrome and digital visual fatigue, with numerous challenges ahead.
The foundation of Science and Humanity is to develop and provide open-ended answers.
The pathogenesis of most ophthalmic conditions is based on genetic and environmental risk factors yet a shift in the importance of genotype versus phenotypic expression under the influence of external and internal causes of an individual definitely took place.
If we use the example of intelligence, as my “genetic masters” Prof. Ewa Bartnik and Prof. Wojciech Dragan say, when we analyze the entire population (from a newborn to the oldest person) the level of heritability of intelligence is 50%, and differences in the influence of genes on intelligence depend on the activity of the environment.
Genetic variances and environmental variances are constantly modifying our pathogenetic cocktails. If we analyze the non-modifiable and modifiable substrates, the last decades and years, in addition to the positive aspects such as extending our lifespan , and remember that age is the primary risk factor for diseases of all kinds, risk factors such as climate change, environmental pollution, changing educational and working conditions, food modifications, widespread consumption of excess calories, especially in the form of highly processed, sweetened products are now critical health challenges, also for the organ of the visual system.
Psychology and especially psychosomatics are also of increasing importance.
Visual perception is another area being explored and tamed.
In a world of artificial intelligence, we still lack an integral view, and currently, all technologies absolutely require reason and humility, and human knowledge. Soon, refractive lens and corneal surgery will move toward modifying the cornea and implanting specific lenses that will adapt their optical properties to our visual requirements, varying lighting, different contrast and dynamic visual work distances. We are very privileged that such a huge technological leap has taken place before our eyes. Education, thanks to new tools and especially the use of the metaverse world, will also be decidedly friendlier.
We have shifted the boundaries of senior age and the age of 40-65 is called maturity and we increasingly speak of old age only after the age of 80.
We mature, develop, age, we are subject to involutionary changes and multiple factors from the day we are born and even throughout our fetal life. This applies to all structures of the eye, but especially significantly to the retina and lens, which processes known as presbyopia are associated with. Keep in mind that it is not a disease, but many conditions can accelerate and intensify this process.
The lens of the human eye is an intraocular structure whose main tasks are active participation in accommodation, refracting light and maintaining clarity. A normal lens, outside of fetal life, is devoid of blood vessels and nerves and is completely transparent. The lens of the eye is a unique structure, and its growth is caused by the addition of new cells inside the surrounding capsule. The new fibers become thickened and fuse with those previously formed. Older cells are not discarded or removed, but placed in its center. This is necessary to maintain the metabolic viability of the outer cortex (and thus the entire organ) and to produce the refractive properties necessary to focus images on the retina and reduce spherical aberration. With age, however, this brings undesirable consequences, including the development and progression of presbyopia.
Presbyopia is not a refractive defect, it is a peculiar indisposition of near vision manifested >40 years of age resulting from widespread involutionary processes. It is caused by physiological anatomical and functional changes occurring in the intraocular lens, especially its capsule, and functional changes in the ligamentous apparatus, resulting in decreasing amplitude of accommodation, i.e. reduced/insufficient ability to sharpen the image of close objects. Interestingly, the strength and work of the ciliary muscle is not affected, thus the full contraction and diastole of this muscle induces adequate changes in the tension of the ligamentous system, and only these forces are met with an altered susceptibility of the lens capsule and the lens itself to respond to a given accommodative stimulus. Such a condition calls for support, i.e. optical correction for nearsightedness. Its recommendation should not be delayed, as procrastination may result in causing symptoms of asthenopia and impaired nearsightedness in the future.
Let’s give our organ of the visual system the best possible correction, let’s use all possible solutions. Our brains like to be given tasks, they like to learn, and if we feed them properly, they will help us use more and more precise, higher resolution correction methods for years to come, as long as we make sure that the plasticity of our brain is preserved.
Dr. Anna M. Ambroziak talks with an invited expert during an interview series entitled “Let’s talk about sight” (#PorozmawiajmyoWzroku) at the Ophthalmology Center Świat Oka in Warsaw.
Can we guard against age-related retinal degeneration? What can we do in this area and, in your opinion, is such knowledge generally available?
The basis of ophthalmology is prevention and age-related maculopathy is a classic example of this. If we have a positive family history and other risk factors besides age, such as nicotinism, atherosclerosis, carbohydrate-lipid disorders, among others, then we should not delay screening and perform it systematically. Age-related macular degeneration (AMD) is the most common cause of so-called “practical blindness” in developed countries, occurring most often in people over 50. It is believed that the incidence of AMD will increase as a result of global population aging. AMD is a degenerative disease that destroys the retina in the place that is the most critical to the vision process – the macula, most often through atrophy of the pigment epithelium, choriocapillaries and photoreceptors and the development of pathological neovascularization. The pathogenetic mechanisms of the disease, described in detail, are indirectly responsible for its early and correct diagnosis. Knowledge of the processes that occur in aging tissues, as well as complex processes caused by external factors and genetic conditions, allow specialists to differentiate the degenerative changes that arise and classify them into different stages of disease development. A number of risk factors, which are divided into modifiable and non-modifiable ones, are subject to analysis both to assess the risk of the onset of the condition and its subsequent progression. Ongoing research on these factors is focusing the attention of specialists on their potential use in prevention and therapy. An interview based on these risk factors provides important information about the patient’s overall health and predisposition to develop maculopathy. In the diagnosis of AMD, there is no single rigid regimen of management, since the disease is not homogeneous and is characterized by a very wide spectrum of symptoms. Among the diagnostic methods described, imaging studies predominate, which can be divided into invasive studies – advanced vascular studies performed by ophthalmologists, and non-invasive studies – imaging degenerative changes, performed by both teams of specialists. Early diagnosis of age-related macular degeneration offers the possibility of preserving the patient’s normal visual function. The progression of untreated disease promotes the development of symptoms whose effects are irreversible.
AMD is an example of a disease in which a holistic view of the entire body is critical. The patient should therefore take full responsibility for his or her health and ensure proper diet and physical activity and not delay a visit to a specialist. Education level is insufficient in every dimension of our physical, mental and social well-being.
One of the world’s most popular imaging diagnostic techniques is optical tomography OCT. Recent research conducted at the International Centre for Translational Eye Research (ICTER) under the supervision of Professor Maciej Wojtkowski have allowed the development of an improved method called Spatio-Temporal Optical Coherence Tomography (STOC-T) that enables imaging of the retina with preserved high-resolution at any depth in the frontal section. The use of STOC-T for retinal imaging makes it possible to reconstruct the morphology of the cones in the human eye. From your point of view, why is retinal imaging important? Which diseases would imaging of the morphology of the cones be crucial for?
OCT is a widely used technology in ophthalmology and allows imaging of all structures of the eyeball, both anterior and posterior, but the greatest research and scientific achievement is in imaging the retina in the central, or macular, area.
Imaging of the morphology of the cones opens a kind of gateway to eternity by enabling anatomical and functional monitoring of photoreceptors that receive visual stimuli and thus informs the first changes leading to, and long before, the onset of maculopathy. It thus provides us with a range of variables for monitoring and modifying perceptual processes, including particularly promising prospects for detecting dementia-like changes and thus accurately assessing cognitive and executive functions.
The key to the future is to capture the state in which the physiological changes that occur in the aging process of eye tissues transform into pathologies.
Dr. Anna M. Ambroziak
For the diagnosis of retinal diseases, not only structural, but also functional changes are important. The group of functional methods includes a precise variant of visual field testing – microperimetry. A novel method is being developed at ICTER: two-photon microperimetry, which takes advantage of the two-photon vision effect occurring when the retina is illuminated by a femtosecond infrared laser pulse. Physics shows that the longer the wavelength of light, the weaker it scatters in the medium. Therefore, in your opinion, can the use of infrared for functional vision testing expand the applicability of microperimetry?
Absolutely yes.
Both in terms of screening in at-risk groups and the broad prevention of macular disease, as well as the standards of management of myopia and glycemic/diabetic disorders.
Comprehensive diagnostic measures performed by ophthalmologists and optometrists are the cornerstone of their daily practice. Complementary examinations performed by both teams are the basis for proper and early diagnosis of many diseases of the visual system and implementation of effective treatment. In the diagnosis of retinal diseases, the range of examinations is very wide and includes both invasive methods and increasingly popular non-invasive examinations, which are expanding the standards of ophthalmic-optometric examinations.
Our research shows that two-photon microperimetry has better repeatability than traditional microperimetry. In your opinion, could this be important for diagnosing eye diseases or tracking their progress? If so, for which diseases in particular?
Absolutely yes.
Precise assessment of the progression of changes over time and high sensitivity and specificity of central perimetry parameters are the greatest challenges of current diagnostics.
Each of the broad spectrum of entities in the maculopathy family requires reproducible data, but myopic maculopathy should definitely be highlighted in this group.
Let’s return to imaging methods by staying with two-photon effects: we are also developing a two-photon variant of fluorescence scanning laser ophthalmoscopy. A standard fluorescence scanning ophthalmoscope (SLO) uses a beam from the visible range, with a wavelength of typically around 480 nm (blue). This wavelength allows to excite the fluorescence of lipofuscin deposits in the pigment epithelium, but not of pigments involved in visual cycle transformations, such as retinyl esters. They are excited with shorter wavelengths, absorbed in the cornea, so it is impossible to detect them with such a standard SLO. The two-photon variant of this device that we are developing at ICTER circumvents this limitation. Do you think this could be an interesting tool for ophthalmologists?
Absolutely yes for the third time. The two-photon effect, as in perimetry, totally changes the perspective and raises the level of reliability of the examinations carried out, which is particularly justified in combination with SLO technology, since it makes it possible to detect changes at the cellular level in the period before the formation of functional changes, such as perimetric changes.
What are the available methods of keratoconus examination? What are their limitations?
First: genetics has entered diagnostics.
Second: imaging is giving us a new generation of tools with increasingly higher resolution and precision.
Corneal cone (Keratoconus, KC) is a bilateral, albeit asymmetric, condition that involves progressive thinning and convexity of the cornea, leading to irregular astigmatism. Keratoconus usually develops in the second or third decade of life. The condition affects all ethnic groups and both sexes. The prevalence and incidence rates of keratoconus can vary by geographic location and age of onset.
Approximately 73% (16 of 22) of human autosomal chromosomes are associated with KC , and 59% of these can be considered to show statistically significant associations (8 of 63). Studies suggest that it may be a polygenic disease, meaning that two or more affected genes are required for the development of keratoconus.
Keratoconus is a multifactorial disease and many genetic factors, along with various external factors, influence phenotypic expression and its development.
And what do we know from the Polish research I have been doing for many years? That is, what do we know about the KC-related protein?
The ALDH3A1 protein is important in maintaining corneal physiology and protecting the eye from UV damage. However, no genome-wide association study has shown that the ALDH3A1 locus is associated with keratoconus. In this study, we investigated the potential role of ALDH3A1 variants as risk factors for the onset and severity of KC in a large group of Polish patients with keratoconus. In the first step, we analyzed the sequence of the coding region of ALDH3A1 in the KC subgroup. We then genotyped three selected ALDH3A1 variants in a larger group of KC patients (n=261) and healthy controls (n=317). We found that the minor A allele of rs1042183 is a risk factor for keratoconus in the dominant model. Genotypes of the rs2228100 variant appear to be associated with an earlier age of KC diagnosis in the Polish population (p=0.055 for the comparison of the three genotypes and p=0.022 for the dominant inheritance model). We showed that the rs1042183 variant in the ALDH3A1 gene is associated with predisposition to keratoconus in the Polish population. The allele frequency of ALDH3A1 variants associated with KC varies in different populations, which may be partly responsible for the difference in KC prevalence worldwide.
Early studies that diagnosed keratoconus were based mainly on symptoms seen on retinoscopy, non-standardized keratometry measurements and subjective assessment of clinical symptoms. Another diagnostic parameter is pachymetry, or corneal thickness assessment. We use different technologies and base the measurements on specific maps.
Until the development of technology and the advent of the ability to diagnose keratoconus with topography and high-resolution optical coherence tomography, information about corneal curvature was provided by keratometry.
Both pachymetry and keratometry are an essential part of the examination performed by an ophthalmologist or optometrist. The measurements obtained during the examination with an autorefractometer, should be the starting point of a comprehensive diagnosis.
Optical coherence tomography is a non-contact and non-invasive method of receiving and then processing an optical signal. It uses superluminescent diodes, which are a source of low-energy infrared light, to image high-resolution structures of the anterior segment of the eye. It is a Swept Source (SS-OCT) device that uses a long-wavelength light source with a central wavelength of 1310 nm and has a speed of 30,000 axial scans per second. The use of long-wavelength light, reduces unwanted scatter, and this results in a greater ability of the light to penetrate opaque structures, i.e. through the sclera or opaque cornea.
The device, performing qualitative analysis of the collected data, forms various types of tomographic and topographic maps of the anterior surface of the eye, the device generates a report respecting the percentage of similarity of the examined patient’s cornea to a typical cone eye model (ESI – Ectasia Screening Interpreted). Anterior corneal curvature and anterior and posterior astigmatism are significantly elevated in a person diagnosed with keratoconus; these parameters are not particularly useful in differentiating subclinical keratoconus from healthy eyes.
Epithelial criteria are the current diagnostic trend.
In daily practice, the usefulness of posterior corneal measurements continues to be emphasized, as changes in the posterior surface of the cornea can be one of the first clinically detectable signs of keratoconus. These measurements could not previously be obtained from traditional reflection-based topographers; they are measured using Scheimpflug imaging and anterior segment optical coherence tomography (AS OCT). By comparing topography maps taken over months and years, a trend curve of the condition is generated, e.g., the Cone Trend Analysis report, which is a key element in assessing the progression of keratoconus repression. A limitation, and thus a diagnostic challenge, is the detection of preclinical cases (pre-KC).
Dr. Anna M. Ambroziak and the Świat Oka Center in Warsaw.
What fields will develop in the next 10 years? What are the biggest challenges for scientists in the field of optics, optometry, ophthalmology and for medical staff specializing in the diagnosis and treatment of eye disorders?
New optics and the use of artificial and augmented intelligence are among the trends, simultaneously, we know more and more about our brain and are pushing the limits of neuroregenerative abilities. Still, the most common cause of decreased visual acuity is uncorrected inaccuracy. The visual organ allows us to perceive stimuli from the surrounding world. Visual sensory fibers have the largest brain representation among our senses, the information transmitted through them, however, requires a very precise receptor. More than half of European adults are diagnosed with refractive errors (myopia≤-0.50, hyperopia ≥+0.75, astigmatism ≥0.75). Everyone over the age of 40, regardless of the type and level of non-massive refraction, needs nearsightedness-support, i.e. correction of presbyopia. Still, despite such modern tools, very often the visual defect is not corrected or is only partially corrected. According to estimates, at least one in two adults should use glasses or contact lenses or another form of correction, but this is not the case. This fact has strong economic implications, both individually and socially, and is a potential cause of decreased productivity and quality of life. I am pointing to significant differences in the assessment of most functions, from overall quality of vision to mental health.
Most of us believe that the primary symptom of an uncorrected vision defect is blurred vision. We see with our brains. The brain selects sharp images, and the eye, thanks to its ability to accommodate, can sharpen the image provided by the impulse. This explains in some cases the ability to read despite the lack of proper correction.
A patient with an uncorrected visual impairment subconsciously seizes the opportunity to minimize the discomfort of a blurry retinal image and squints. Narrowing the eyelid crevice restricts the access of rays that run off-axis through the optical system of the eye. Light rays that enter the receptors in the retina when the eyelids are closed run axially and have a much smaller effect on blurring the image than off-axis rays. By squinting, a person with a refractive defect makes the image they see clearer, but is still subject to the typical symptoms of asthenopia, which is a reaction of the visual system to increased visual effort caused by an uncorrected refractive defect, most often hyperopia and astigmatism. Other causes of asthenopia can be phoria, which is a misalignment disorder of binocular vision, convergence or accommodative disorders.
There are a number of mechanisms in the human visual system that offset the discomfort caused by visual defects or disorders of the visual system, including fusiform vergence or accommodations. These mechanisms can become impaired during illness, under stress or as a result of intensive visual work at close distances.
The discomforts associated with uncorrected or undercorrected visual impairment are usually not sudden in nature and do not cause ocular signs for a long time. Their occurrence is often read in terms of somatic disorders manifested, for example, by general fatigue, irritability, dizziness or headaches. We should discuss this with our patients. Adequate optimization of retinal and cerebral images expands the doors of perception and thus future possibilities for intraocular correction and neuroadaptation to modern optics.
Let us take care of the psyche and help the brain refine the senses.
My dream is education, education addressed to us – specialists, education of our patients, education of their families, education of officials and decision-makers. My dream is for patients to benefit and be aware of the need for prevention. I know this sounds like utopia to realists, but this is my reality, and I want to share it. We are the ones who create reality! If only we start with small steps, with small things, with examples, with ourselves and our own backyard and realize this ideal world. Just as in Świat Oka we showed the space for eye care professionals to work together. This is the only way we can change our reality. First of all, the environment! Our polluted world is the starting point for autoimmune diseases, and diseases on the spectrum are not only ophthalmic and ocular surface. Our contaminated air, water and soil and the lack of natural light for our young people, our children and teenagers means obesity and being overweight, it means myopia. These diseases already affect half the population of young people and their numbers are increasing dramatically. Psychosomatic diseases constitute now about 70-80% of diseases, autoimmune diseases similarly. The number of people requiring vision correction and vision therapy is similar and so few, far less than half, benefit from it. The majority of parents (more than 80%) believe, and this is us who is responsible for this educational error, that children only require vision control when they start going to school. Many still do not understand that a full Optometric and Ophthalmic examination is the basis, and we are not talking about any exceptionally high standards. At least two hours in natural light and dietary changes are the basis for holistic management of our patients of all ages. Digital eye fatigue along with disorders of the ocular surface, disorders of convergence, accommodation, with visual defects. including pseudo-short-sightedness simply require attentiveness, awareness of here and now, and willingness. No exceptional solutions or finances are needed there. Our dream for the present is for us to get examined and undergo corrections when needed. We will then be able to let our tired and irritated minds rest. The next step is modern diagnosis and treatment of ophthalmic conditions.
Eye screening programs are still needed both in developing countries and here in the center of Europe, where preventive care in ophthalmology still does not happen realistically.
Interview questions prepared by: Marta Mikuła-Zdańkowska, PhD and Oliwia Kaczkoś, MSc.
Expert supervision: senior researcher Katarzyna Komar, PhD.
Additional contribution: Anna Salamończyk.
THE INTERVIEW WAS REALIZED BY THE MEMBERS OF THE PHYSICAL OPTICS AND BIOPHOTONICS GROUP LED BY PROF. MACIEJ WOJTKOWSKI, HEAD OF ICTER.
Manage Cookie Consent
We use cookies to optimize our website and our service.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.